Background
Rotator cuff injuries are a common cause of shoulder pain in people of all age groups. They represent a spectrum of disease, ranging from acute reversible tendinitis to massive tears involving the supraspinatus, infraspinatus, and subscapularis. Diagnosis is usually made through detailed history, physical examination, and often, imaging studies.[1, 2, 3, 4, 5]
A normal rotator cuff and rotator cuff tear are shown below.
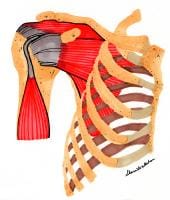 Rotator cuff, normal anatomy.
Rotator cuff, normal anatomy.  Rotator cuff tear, anterior view.
Rotator cuff tear, anterior view. Often, younger individuals with rotator cuff injuries relate a history of repetitive overhead activities involving the rotator cuff or, less commonly, a history of trauma preceding clinical onset of symptoms. In contrast, older individuals usually present with a gradual onset of shoulder pain and, ultimately, after radiographic testing is shown to have significant partial or full rotator cuff tears without a clear history of predisposing trauma. Nonoperative or conservative treatment is usually sufficient to heal the problem in the vast majority of individuals, with a few exceptions that are discussed.[1, 2, 3, 4, 5]
For excellent patient education resources, see eMedicineHealth's patient education articles Rotator Cuff Injury and Shoulder and Neck Pain.
NextEpidemiologyFrequencyUnited StatesThe frequency of full-thickness rotator cuff tears ranges from 5-40%, with an increasing incidence of cuff pathology in advanced age. Cadaveric studies by Bigliani et al found that 39% of individuals older than 60 years had full-thickness rotator cuff tears with an even higher incidence of partial tears.[6]
PreviousNextFunctional AnatomyNormal shoulder motionThe shoulder complex is comprised of several joints, including the sternoclavicular joint, acromioclavicular joint, glenohumeral (GH) joint, and scapulothoracic (ST) joint or pseudoarticulation. These articulations work together to carry out normal shoulder motion. The majority of motion occurs at the GH and ST joints. A rhythm between these 2 areas of motion has been described.[1, 3, 7, 8, 9, 10, 11, 12]
The GH–to–ST motion ratio of total shoulder motion is 2:1 (ie, 180° of abduction, consisting of 120° of GH motion and 60° of ST motion). The 2:1 ratio is an average over the entire arc of motion. This ratio changes through the arc of motion (ie, the 2:1 ratio is not constant throughout the entire range of motion [ROM]). In the initial portion of abduction, GH motion predominates and the ratio is 4:1 (GH:ST). As the shoulder moves above 90° of abduction, this ratio becomes 1:1° GH to 1° ST motion.
The importance of the scapula in normal shoulder motion cannot be overstated. The scapula, with the glenoid as its contact point, forms the platform for humeral head articulation and motion. A stable platform is essential for normal shoulder biomechanics in everyday activities and is crucial for high-demand activities (eg, overhead sports or work).[13]
The scapula must glide along the chest wall as it protracts and retracts during normal shoulder movements. Scapular winging results in glenoid antetilting, which results in functional elevation of the humeral head and impingement of the rotator cuff. In addition, without scapular motion, the origin and insertion of the deltoid approximate each other, resulting in a decreased optimal length-tension relationship and a decrease in force as the shoulder abducts. Normal scapular motion allows the deltoid to maintain its length-tension relationship and generate adequate force.
Stabilizers of the shoulderThe shoulder is considered a ball-in-socket joint, although the glenoid fossa is flat. In addition, the surface area of the glenoid is much smaller than that of the contacting humeral head (25-30%). The cartilaginous labrum provides much of the socket function and increases the surface area of contact for the humeral head.
Together, these components provide a great amount of shoulder mobility with limited stability. Shoulder stabilizers can be grossly categorized as static or dynamic. Dynamic stabilizers require an intact neuromuscular system to function, whereas static stabilizers help maintain congruity.
The static stabilizers have been studied well in cadaver specimens to understand their stabilizing effects. Static stabilizers continue to function in the setting of neurologic or intrinsic muscle pathology in conditions such as hemiplegia, spinal cord injury, brachial plexus injury, suprascapular nerve injury, and myopathies. This is not true for the dynamic stabilizers (eg, rotator cuff muscles). With neuromuscular injury or intrinsic muscle damage, the dynamic stabilizers lose their ability to exert dynamic motor control of the humeral head, ultimately leading to GH laxity and shoulder pain.
Static stabilizersStatic stabilizers include the bony structures, labrum, GH ligaments, and joint capsule. Unlike the hip joint, the bony articulation of the shoulder offers little stability. This is due to the limited contact area of the glenoid with the humeral head, flattened architecture, and retroverted positioning. The labrum is a fibrous structure that attaches to the glenoid to increase the contact area and deepen the socket of the glenoid up to 50%, forming a concave surface. Three GH ligaments exist, as follows: superior, middle, and inferior. The inferior GH ligament is the most important for shoulder stability and has 3 components, anterior, inferior, and posterior, therefore, it is more appropriately referred to as the inferior GH complex.
Dynamic stabilizersDynamic stabilizers[14] include the rotator and scapular stabilizers (ie, teres major, rhomboids, serratus anterior, trapezius, levator scapula). The rotator cuff is composed of 4 muscles: the supraspinatus, infraspinatus, subscapularis, and teres minor. The supraspinatus is the principal supporting and kinetic muscle of the shoulder. The primary function of the rotator cuff muscles is to stabilize the GH joint so that the larger shoulder movers (eg, deltoid, latissimus dorsi) can carry out their function without significant motion of the humeral head on the glenoid. Increased movement results in shearing forces across the joint (to the labrum, in particular) and may result in humeral head migration and impingement upon the rotator cuff muscles and tendons.
The rotator cuff muscles are associated and assist with some shoulder motion; however, their main function is to provide stability to the joint by compressing the humeral head on the glenoid. The supraspinatus assists in shoulder abduction by maintaining the humeral head centered on the glenoid, with the middle deltoid acting as the primary mover. These muscles act as force couples, because they work synergistically to carry out a particular movement.
Electromyography (EMG) studies have demonstrated a high degree of supraspinatus activity during the initial 30° of abduction. This has been misinterpreted to imply that the supraspinatus initiates shoulder abduction and acts to abduct the shoulder in the first 30°. In actuality, the supraspinatus fires to stabilize the GH joint as the deltoid abducts the arm.[15, 16, 17, 18, 19]
Increased EMG activity in the supraspinatus during the initial 30° is a reflection of increased firing requirements of this muscle to stabilize the GH joint as the deltoid is activated. The infraspinatus and teres minor muscles assist in external rotation of the shoulder and also provide an inferior pull upon the humeral head, assisting in its centering during overhead activity. The subscapularis muscle participates in this centering but also acts with the pectoralis muscles and latissimus dorsi as an internal rotator of the shoulder, serving as the main internal rotators of the shoulder.
Weakness or insufficiency of the rotator cuff muscles results in increasing demands on the static stabilizers. If these demands are long term or recurrent, static stabilizers may begin to fail. This can result in stretching or attenuation of the capsule, which results in even greater shoulder laxity and greater demands on the already weak rotator cuff muscles. Humeral head migration may occur with capsule laxity and result in rotator cuff impingement and pain. Pain may inhibit rotator cuff muscle firing, leading to disuse and further weakening of the dynamic stabilizers with greater demands placed on the static stabilizers.
Increased humeral head translation can also lead to shearing and injury to the glenoid labrum. Rotator cuff impingement, tendinitis, and labral pathology are commonly encountered injury patterns in athletes and workers who perform overhead motions. Focusing solely on the static stabilizers in treatment neglects the dynamic structures that probably initiate and perpetuate the cycle.
PreviousNextSport-Specific BiomechanicsA similar type of motion is involved in a number of overhead sports activities (eg, serving in tennis, spiking in volleyball, throwing a football or baseball). The baseball throwing motion has been studied in detail and can be divided into 5 stages.
Stage 1 is the wind-up phase. EMG studies have determined that the rotator cuff muscles are inactive during this initial stage.Stage 2 is the early cocking stage and involves shoulder external rotation and abduction supplied primarily by the deltoid.Stage 3 is the late cocking stage, which continues until maximal external rotation is achieved. The rotator cuff muscles are very active during this stage, especially the subscapularis, which eccentrically contracts and acts as a dynamic stabilizer. Stage 4 is the acceleration stage, which begins with internal rotation of the humerus and ends with release of the baseball. During this phase, the pectoralis major and the latissimus dorsi are very active, whereas the muscles of the rotator cuff are inactive. Stage 5 is the follow-through of the baseball pitch, where deceleration takes place. During this phase, the rotator cuff muscles and the posterior deltoid are most active. The supraspinatus eccentrically contracts to decelerate internal rotation of the limb.Proper balance between the concentrically contracting muscles that generate force and the eccentrically contracting muscles that control movement is important. Imbalance between these opposing muscle groups results in overuse of muscles and, ultimately, overuse injuries of the shoulder. Note that a great deal of the force generated in overhead sports occurs in the trunk and lower extremity, and these areas should be targeted in any conditioning program for athletes who throw.
PreviousProceed to Clinical Presentation , Rotator Cuff Injury





0 comments:
Post a Comment
Note: Only a member of this blog may post a comment.