Background
Injuries to the lumbar spine have received only a small amount of attention compared with other athletic injuries. This can be explained by a number of reasons. Spinal fractures are relatively uncommon in sports participation compared with other types of injuries; most injuries to the lumbar spine are relatively minor and fit into the category of soft-tissue injuries. These soft-tissue injuries are usually self-limited and resolve without coming to the attention of healthcare professionals.
The mechanisms and severity of sports-related lumbar spinal injuries reflect a competitive and risk-taking culture.[1, 2, 3, 4, 5, 6] Lumbar spine bony injuries are often limited to specific sports, most frequently seen in sports such as automobile or motorcycle racing,[7, 8, 9] skydiving[10] (see the image below), power weight lifting,[11, 12] wrestling,[13] gymnastics,[14, 15, 16] football,[17, 18, 19, 20, 21, 22] hockey,[23] rowing,[24] horseback riding,[25, 26] and high-speed snow sports.[27, 28, 29, 30, 31] This article reviews the diagnosis and management of acute lumbar vertebral fractures.
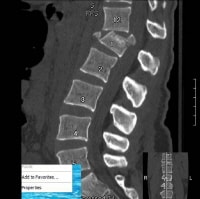 Sagittal computed tomography scan reconstruction of a young female who had a skydiving accident. The parachute deployed, but the patient landed on concrete and sustained a lower-extremity fracture and a fracture of L1. She was neurologically intact but required an open reduction with a fusion and instrumental fixation of the fracture.
Sagittal computed tomography scan reconstruction of a young female who had a skydiving accident. The parachute deployed, but the patient landed on concrete and sustained a lower-extremity fracture and a fracture of L1. She was neurologically intact but required an open reduction with a fusion and instrumental fixation of the fracture. For excellent patient education resources, see eMedicineHealth's patient education articles Vertebral Compression Fracture and Low Back Pain.
Related Medscape Reference topics:
Lumbar Disk Problems in the Athlete
Lumbar Spine Fractures and Dislocations
Lumbar Spine Trauma Imaging
Lumbosacral Disc Injuries
Lumbosacral Discogenic Pain Syndrome
Related Medscape resources:
Resource Center Exercise and Sports Medicine
Resource Center Joint Disorders
Resource Center Spinal Disorders
CME/CEÂ Back Pain in a 39-Year-Old Man from Guatemala
CMEÂ Early Surgery for Severe Sciatica Relieves Pain Faster Than Conservative Treatment
CME/CEÂ Low Back Pain: Evaluating Presenting Symptoms in Elderly Patients
NextEpidemiologyFrequencyUnited StatesThe epidemiology of thoracic and lumbar spine injuries in athletes is very difficult to document. Most epidemiologic studies on lumbar spine injuries in athletes lack prospective data. The thoracolumbar junction and lumbar spine are common sites for fractures due to the high mobility of the lumbar spine compared with the more rigid thoracic spine. Injury to the cord or cauda equina occurs in approximately 10-38% of adult thoracolumbar fractures and in as many as 50-60% of fracture dislocations. The rate of bony injury without neurologic consequence is undoubtedly higher.
In the United States, Keene reported an overall rate of 7% for sport-related lumbar injuries in the athlete population.[30] Most of these injuries occurred during practice or preseason conditioning, and only 6% occurred during actual competition. Lumbar spine injuries were significantly more common in football[17, 18, 19, 20] and gymnastics.[14, 15, 16]
Statistics from the US Air Force Academy indicated that 9% of all athletic injuries affect the spinal column. In an analysis of injuries in a professional football team, Ryan et al reported a 6% rate of spinal injuries.[9] Snook reviewed all musculoskeletal injuries sustained by college wrestlers and female gymnasts and found a rate of thoracolumbar spine injuries of 2% for the wrestlers[13] and 13% for the female gymnasts.[32]
Related Medscape Reference topics:
Cauda Equina and Conus Medullaris Syndromes
Lumbosacral Facet Syndrome
Lumbosacral Radiculopathy
Lumbosacral Spondylolisthesis
Lumbosacral Spondylolysis
Related Medscape resources:
Resource Center Exercise and Sports Medicine
Resource Center Osteoporosis
Specialty Site Orthopaedics
InternationalInformation on the incidence of sports-related spinal injuries in other countries is also limited and difficult to determine due to differences in data collection and reporting among countries. In England, Williams estimated that spinal injuries accounted for 15% of all injuries sustained in sports.[10] Furthermore, injuries to the thoracic and lumbar spine seemed to be more frequent in automobile racing, horseback riding, parachuting, mountain climbing, and weightlifting.
PreviousNextFunctional AnatomyThe lumbar spine consists of a mobile segment of 5 vertebrae, located between the relatively immobile segments of the thoracic and sacral segments at either end. The thoracic spine is stabilized by the attached rib cage and intercostal musculature, whereas the sacral segments are fused, providing a stable articulation with the ilium. The lumbar vertebrae are particularly large and heavy compared with the cervical and thoracic vertebrae. The bodies are wider, the pedicles are shorter and heavier, and the transverse processes project somewhat more laterally and ventrally when compared with other spinal segments. The laminae are shorter vertically than the bodies and are bridged by strong ligaments. Finally, the spinal processes are broader and stronger than those in the thoracic and cervical spine.[33]
The lumbar spine must transmit compressive, bending, and twisting forces that are generated between the upper and lower body. Consequently, as one moves more caudally into the lumbar spine, the muscle groups and ligaments become larger and stronger.
The intervertebral discs consist of 2 components, the annulus fibrosus and the nucleus pulposus. The annulus is a dense fibrous ring located at the periphery of the disc, which has strong attachments to the vertebrae and serves to confine the nucleus pulposus. The lumbar spine is surrounded by powerful musculature and ligaments, which dynamically stabilize the spine.
Related Medscape Reference topic:
Topographic and Functional Anatomy of the Spinal Cord
PreviousNextSport-Specific BiomechanicsThe lumbar spine is a complex, 3-dimensional (3-D) structure that is capable of flexion, extension, lateral bending, and rotation. In the spine, the total range of motion is the result of a summation of the limited movements that occur between the individual vertebrae. Strong muscles and ligaments are crucial for supporting the bony structures and for initiating and controlling movement.
The most common movement of the lumbar spine is flexion. During flexion, anterior compression of the intervertebral disc and widening of the spinal canal occurs along with some sliding movement of the articular process in the zygapophyseal joint. This movement is limited by the posterior ligamentous complex and the dorsal muscles. Extension of the lumbar spine is more limited, producing posterior compression on the disc, narrowing of the spinal canal, and a sliding motion of the zygapophyseal joint. The anterior longitudinal ligament, ventral muscles, lamina, and spinous processes limit the extension of the lumbar spine.
Lateral bending involves lateral compression of the intervertebral disc, along with sliding separation of the zygapophyseal joint on the convex side. An overriding of the zygapophyseal joint occurs on the concave side. The intertransverse ligaments limit the lateral bending of the spine. Rotation of the lumbar spine involves compression of the annulus fibrosus fibers. It is limited by the geometry of the facet joints and the iliolumbar ligaments. The motion of the lumbar spine cannot be considered without evaluating the synchronous movements of the cervical and thoracic spine. The entire spinal column moves as one unit in all planes of motion. Each region of the spine has its own characteristic curvature. These curves allow an upright posture while maintaining the center of gravity over the pelvis and lower limbs. Although most rotation is accomplished at the cervical spine, flexion and lateral bending are primarily cervical and lumbar functions.
Spinous process fractures may occur as a result of direct trauma to the posterior spine or as a result of forcible flexion and rotation. These injuries are usually not associated with neurologic deficits. Violent muscular contraction or direct trauma can cause fractures of the transverse processes. For example, a football helmet blow to the back can cause fractures of either the spinous or transverse processes. Burst fractures (see the images below) are usually associated with axial loading and compression of the spine. Acute traumatic spondylolisthesis is usually associated with major trauma and extreme hyperextension of the spine.
 Sagittal T1-weighted magnetic resonance imaging study of a professional driver who was in a rollover motor vehicle accident while racing his car. This figure shows a T-10 unstable burst fracture producing severe kyphotic deformity of the spine. The abnormal signal on the vertebral body and the extradural defect represents a subacute hematoma producing spinal cord compression. The patient had severe paraparesis and underwent an emergency operation. The procedure involved an anterolateral retroperitoneal approach with a corpectomy and vertebral reconstruction.
Sagittal T1-weighted magnetic resonance imaging study of a professional driver who was in a rollover motor vehicle accident while racing his car. This figure shows a T-10 unstable burst fracture producing severe kyphotic deformity of the spine. The abnormal signal on the vertebral body and the extradural defect represents a subacute hematoma producing spinal cord compression. The patient had severe paraparesis and underwent an emergency operation. The procedure involved an anterolateral retroperitoneal approach with a corpectomy and vertebral reconstruction.  Postoperative plain x-ray film of a professional driver who experienced a burst fracture in a rollover motor vehicle accident while racing his car. This image shows a vertebral reconstruction with the use of a titanium cage filled with bone and the arthrodesis with a Z plate.
Postoperative plain x-ray film of a professional driver who experienced a burst fracture in a rollover motor vehicle accident while racing his car. This image shows a vertebral reconstruction with the use of a titanium cage filled with bone and the arthrodesis with a Z plate. 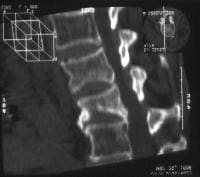 Sagittal computed tomography scan reconstruction of an athlete who had a burst fracture.
Sagittal computed tomography scan reconstruction of an athlete who had a burst fracture. The intervertebral discs are thick and strong. The annulus fibrosus receives most of the forces that are transmitted from one vertebral body to another, and it is designed to resist tension and shearing forces. The nucleus pulposus is designed to resist compression forces; it receives primarily vertical forces from the vertebral bodies and redistributes them in a radial fashion to the horizontal plane. This structure allows the intervertebral discs to dissipate the axial loading.
Related Medscape Reference topics:
Disk Herniation Imaging
Herniated Nucleus Pulposus
Lumbar Compression Fracture
Lumbosacral Spine Sprain/Strain Injuries
Lumbosacral Spondylolisthesis
Lumbosacral Spondylolysis
Related Medscape resources:
Resource Center Spinal Disorders
Specialty Site Neurology & Neurosurgery
Specialty Site Orthopaedics
PreviousProceed to Clinical Presentation , Lumbosacral Spine Acute Bony Injuries





0 comments:
Post a Comment
Note: Only a member of this blog may post a comment.