Background
Thoracic outlet syndrome is not the name of a single entity, but rather a collective title for a variety of conditions attributed to compression of these neurovascular structures as they traverse the thoracic outlet.[1, 2, 3, 4, 5] The thoracic outlet is bordered by the scalene muscles, first rib, and clavicle. Neurovascular structures pass from the neck and thorax into the axilla through this space. Thoracic outlet syndrome remains one of the most controversial clinical entities in medicine.[6, 7, 8] See the image below.
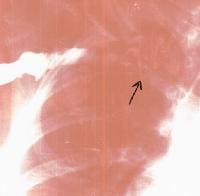 Thoracic outlet syndrome in a 16-year-old volleyball player with a stenotic right subclavian vein (arrow) secondary to fibrosis.
Thoracic outlet syndrome in a 16-year-old volleyball player with a stenotic right subclavian vein (arrow) secondary to fibrosis. For excellent patient education resources, see eMedicineHealth's patient education articles Shoulder and Neck Pain and Electromyography (EMG).
NextEpidemiologyFrequencyUnited StatesThe wide variability of symptoms and signs in patients with thoracic outlet syndrome and the lack of an objective confirmatory test for the diagnosis makes correctly identifying patients with thoracic outlet syndrome difficult.[9] Therefore, determining its exact incidence remains elusive; estimates range from 3-80 cases per 1000 population.[10] Thoracic outlet syndrome is more common in women, particularly those with poor muscular development, poor posture, or both.[11]
PreviousNextFunctional AnatomyThe neurovascular bundle courses through 3 spaces, or triangles, as it exits the neck to reach the axilla and proximal arm. All 3 spaces can be the source of compression of the various components of the neurovascular bundle, including the brachial plexus and the subclavian vessels.[12] These spaces are small at rest and become even smaller with certain arm maneuvers, such as abduction and external rotation.[13, 14] This can aid in the diagnosis of thoracic outlet syndrome and forms the basis for provocative testing, which is discussed later (see Clinical, Physical).
The first space is the interscalene triangle. It is bordered by the anterior scalene muscle, the middle scalene muscle, and the upper border of the first rib. This space contains the trunks of the brachial plexus and subclavian artery. The interscalene triangle is the most common site for neural compression, vascular compression, or both.[10]
The second space is the costoclavicular triangle, which is bordered by the clavicle, first rib, and scapula and contains the subclavian artery and vein and the brachial nerves.
The third and final space is beneath the coracoid process just deep to the pectoralis minor tendon; it is referred to as the subcoracoid space.
PreviousNextSport-Specific BiomechanicsThoracic outlet syndrome is most often seen in patients who engage in repetitive motions that place the shoulder at the extreme of abduction and external rotation. An example of such activity is swimming, especially with the freestyle stroke, butterfly stroke, and backstroke. When a swimmer reports tightness and pain around the shoulder, neck, and clavicle as his or her hand enters the water, thoracic outlet syndrome should be suspected.
In addition to swimmers, other athletes affected by thoracic outlet syndrome include water polo, baseball, and tennis players and athletes in any other activity that places repetitive stress on the shoulder at the extremes of abduction and external rotation. These individuals may present with neurologic and arterial or venous symptoms. Venous thoracic outlet syndrome most commonly develops in young male athletes in whom the upper extremity musculature is overdeveloped as a result of work or physical conditioning. Baseball players, whose sport requires repetitive throwing motions, are at increased risk for arterial thoracic outlet syndrome in their dominant arm.
PreviousProceed to Clinical Presentation , Thoracic Outlet Syndrome





0 comments:
Post a Comment
Note: Only a member of this blog may post a comment.