Background
Shoulder dislocations may occur from a traumatic injury or from loose capsular ligaments. Different conditions may affect the stabilizing structures of the shoulder and, thus, negatively affect patients with shoulder dislocations.[1]
Note the images below.
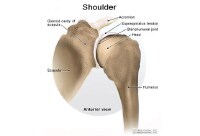 Normal shoulder.
Normal shoulder.  Anterior dislocation.
Anterior dislocation. This article focuses on glenohumeral joint dislocation. Although acromioclavicular (AC) joint separations are sometimes called shoulder dislocations by nonmedical persons, these are not true shoulder dislocations. Shoulder dislocations occur when the head of the humerus comes out of its socket, the glenoid.
For patient education resources, see the Breaks, Fractures, and Dislocations Center and Sports Injury Center, as well as Shoulder Dislocation and Shoulder Separation.
Related Medscape Reference topics include the following:
Acromioclavicular InjuryAcromioclavicular Joint SeparationsDislocation, ShoulderSuperior Labrum LesionsNextEpidemiologyFrequencyUnited StatesThe shoulder is the most commonly dislocated joint in the body.[1, 2, 3]
Although most shoulder dislocations occur anteriorly, they may also occur posteriorly, inferiorly, or anterior-superiorly.
Patients with a previous shoulder dislocation are more prone to redislocation.
Other factors that show a clear correlation to redislocation are the age of the patient and concomitant rotator cuff tears and fractures of the glenoid.
Younger patients (teenagers and those aged 20 years) have a much higher frequency of redislocation than patients in their 50s and 60s.[4] Many physicians believe that age is less of a predisposing risk factor for redislocation than activity level.
Patients who tear their rotator cuffs or fracture the glenoid during their shoulder dislocation have a higher incidence of redislocation than patients without these problems.
PreviousNextFunctional AnatomyShoulder stability is maintained by the glenohumeral ligaments, the joint capsule, the rotator cuff muscles, the negative intra-articular pressure, and the bony/cartilaginous anatomy.
The main stabilizers of the shoulder joint are the ligaments and the capsule complex. Multiple ligaments are present, but the inferior glenohumeral ligament is the most important and the one most commonly injured during an anterior shoulder dislocation. The injury may be a tear of the ligament/capsule off one of its bony attachments, and/or it may cause a stretch injury to these structures.
Tears in the rotator cuff muscles may also lead to shoulder instability. Four rotator cuff muscles are present in the shoulder. They are found superficial to the glenohumeral ligaments and the bones. Large tears may lead to shoulder instability, even with intact glenohumeral ligaments. Instability of the shoulder can also occur from injury to the nerves that control the shoulder muscles, specifically the axillary nerve.
PreviousNextSport-Specific BiomechanicsThe shoulder is a very mobile joint; therefore, it is often placed in awkward positions during sports. Thus, the force from a fall or a blow may be sufficient to cause shoulder damage. If the force is strong enough, the athlete tears the ligaments/tendons, fractures the glenoid or humerus, and dislocates the shoulder.
PreviousProceed to Clinical Presentation , Shoulder Dislocation





0 comments:
Post a Comment
Note: Only a member of this blog may post a comment.