Background
Blazina et al first used the term jumper's knee (patellar tendinopathy, patellar tendinosis, patellar tendinitis) in 1973 to describe an insertional tendinopathy seen in skeletally mature athletes,[1] although Sinding-Larson, Johansson, and Smillie once described this condition. Jumper's knee usually affects the attachment of the patellar tendon to the inferior patellar pole. The definition was subsequently widened to include tendinopathy of the attachment of the quadriceps tendon to the superior patellar pole or tendinopathy of the attachment of the patellar tendon to the anterior tuberosity of the tibia. The term jumper's knee implies functional stress overload due to jumping (see image below).
 The proximal patellar tendon is most commonly affected in jumper's knee.
The proximal patellar tendon is most commonly affected in jumper's knee. For excellent patient education resources, visit eMedicineHealth's First Aid and Injuries Center. Also, see eMedicineHealth's patient education articles Knee Pain Overview, Knee Injury, and Tendinitis.
NextEpidemiologyFrequencyUnited StatesJumper's knee is certainly one of the more common tendinopathies affecting skeletally mature athletes, occurring in as many as 20% of jumping athletes. With regard to bilateral tendinopathy, males and females are equally affected. With regard to unilateral tendinopathy, the male-to-female ratio is 2:1.
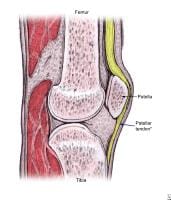
PreviousNextFunctional AnatomyThe rectus femoris and 3 vasti muscles (ie, the vastus medialis, vastus lateralis, and vastus intermedius muscles) join in a common quadriceps tendon that inserts on the patella, the largest sesamoid bone in the human body. This same tendon is known as the patellar tendon from the inferior pole of the patella to its distal insertion at the tibial tuberosity.
Radiologic and histologic studies have shown that the posterior proximal fibers of the patellar tendon appear to be most commonly affected in jumper's knee.[2] Counter to these findings, however, biomechanical research has demonstrated that these posterior fibers can withstand greater tensile strains before failing, compared with the anterior fibers.[3]
PreviousNextSport-Specific BiomechanicsRisk factors and biomechanicsJumper's knee is believed to be caused by repetitive stress placed on the patellar or quadriceps tendon during jumping. It is an injury specific to athletes, particularly those participating in jumping sports such as basketball,[4, 5, 6, 7, 8] volleyball,[7, 8, 9, 10] or high or long jumping.[7, 10] Jumper's knee is occasionally found in soccer players, and in rare cases, it may be seen in athletes in nonjumping sports, such as weight lifting and cycling.
Investigators have implicated sex, greater body weight, genu varum and genu valgum, an increased Q angle, patella alta and patella baja, and limb-length inequality as intrinsic risk factors.[11] However, the only biomechanical impairment prospectively linked to jumper's knee is poor quadriceps and hamstring flexibility.
Vertical jump ability, as well as jumping and landing technique, are believed to influence tendon loading.[4, 10, 12] Volleyball players with a natural ability for jumping high are at increased risk for developing jumper's knee.[13]
In a cohort of elite young volleyball players, male sex, volume of training, and match exposure were all noted to be risk factors. One third of boys aged 16-18 years developed the condition compared with 8% of girls.[14] In a cross-sectional survey of 891 nonelite athletes in the Netherlands, the prevalence of jumper's knee varied from 14.4% and 2.5% for different sports (eg, basketball, volleyball, handball, korfball, soccer, field hockey, and track and field). Younger age, taller body stature, higher body weight, and sport-specific loading characteristics of the knee extensor apparatus were all risk factors for developing jumper's knee.[15]
Overtraining and playing on hard surfaces have been implicated as extrinsic risk factors.
Interestingly, the patellar tendon experiences greater mechanical load during landing than during jumping because of the eccentric muscle contraction of the quadriceps. Therefore, eccentric muscle action during landing, rather than concentric muscle contraction during jumping, may exert the tensile loads that lead to injury.[16]
PreviousProceed to Clinical Presentation , Jumper's Knee





0 comments:
Post a Comment
Note: Only a member of this blog may post a comment.