background
Hand dislocation is a common damage in sports activities and in occupational settings, incessantly appearing to be minor. If the athlete, trainer, or show has already reduced the dislocation, it appears unimpressive when put next with an incredible knee damage or a shoulder dislocation.
however, hand dislocations have actual potential for long-time period incapacity in sports activities and other areas of existence if enough discount is not carried out, if associated injuries are not recognized and as it should be handled or referred, and if doable issues of the damage and its therapy aren't foreseen. The judgment of the initial treating medical doctor may also be crucial in determining the lengthy-time period outcome of these accidents.
Many hand dislocations will also be successfully handled with closed discount, traction, or each. Grossly unstable joints and people for which closed discount has failed most often require surgical intervention. physical and occupational therapy are key elements of therapy all through. Any long-term problems (usually involving stiffness or instability) that improve must be addressed.
NextAnatomyInterphalangeal jointsThe bony anatomy of the proximal interphalangeal (PIP) joint includes medial and lateral condyles on the proximal phalanx, with matching concavities on the associated distal phalanx. The joint has a variety of motion (ROM) in flexion and extension but is moderately rigid in abduction and adduction; hence, it is a hinge (ginglymus) joint functionally. The bony anatomy of the distal interphalangeal (DIP) joint is an identical, but the surrounding soft tissue gives extra restriction in flexion.
The extrinsic flexors across each joints are as a minimum four occasions greater than the extensors, permitting flexion contractures to strengthen very abruptly, especially with immobilization in flexion. sufficient ROM, particularly at the PIP joint, is critical for normal hand function.
The PIP and DIP joints are both supported on all 4 sides by using an identical tender-tissue buildings, which embody the volar plate on the palmar side (the integrity of which is essential for a secure reduction), collateral ligaments on the radial and ulnar sides, and the extensor complicated (vital slip, lateral bands, and hood) dorsally (see the image under). These buildings connect to and beef up the joint tablet. For a dislocation to occur, at least 1, regularly 2, and sometimes 3 of those constructions have to be considerably injured.
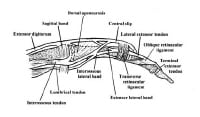 Lateral view of relevant finger anatomy.
Lateral view of relevant finger anatomy. The volar plate is a roughly triangular structure with its base oriented distally, attaching to the volar base of the center phalanx with its tip attaching to the distal facet of the proximal phalanx. The volar plate features generally in limiting hyperextension. to that end, it's just about at all times injured in dorsal dislocations.
The collateral ligaments restrict the joint from opening to varus or valgus stress and are additionally commonly injured in dorsal dislocation. injury to the radial collateral ligament is about 6 occasions more fashionable than harm to the ulnar collateral ligament.
The extensor complex comprises the imperative slip, which attaches to the base of the middle phalanx; the lateral bands, which run dorsolaterally on each and every aspect; and the transverse retinacular ligament, which connects these buildings and extends laterally. It helps restrict volar movement of the base of the center phalanx and subsequently is frequently injured in volar dislocations at the PIP joint, with the center phalanx both tearing the principal slip from its insertion or buttonholing throughout the transverse retinacular ligament between the significant slip and a lateral band.
Metacarpophalangeal jointThe metacarpophalangeal (MCP) joint is regarded as an ellipsoid joint. the head of the metacarpal includes medial and lateral condyles and is narrower on its dorsal floor than on its palmar floor; it fits into the concavity of the bottom of the proximal phalanx. The true collateral ligament attaches to a recess created by the junction of the shoulder and head. The collateral ligament is composed of the next 2 elements:
A dorsally positioned twine portionA fan-formed volar portion or accessory collateral ligament, which extends from the metacarpal to the perimeters of the volar plateto accomplish flexion and extension on the MCP joint, the anterior and posterior components of the tablet should be lax. When the joint is prolonged, the phalanges have substantial lateral play in abduction and adduction; in consequence, this joint shouldn't be regularly injured. on the other hand, if the ligament is torn, dislocation happens.
The MCP joint of the thumb has radial and ulnar collateral ligaments, which might be loose when the joint is prolonged and tight when flexed. When the joint is extended, the proximal phalanx has the lateral play finished by way of the motion of the interosseous muscles.
When the thumb is flexed and in a practical position, as in the case of many sports activities eventualities (eg, snowboarding, falls on a gloved hand), the ulnar collateral ligament is the structure in danger and will also be ruptured (see Skier’s Thumb). The ulnar collateral ligament can then be displaced in order that the adductor aponeurosis is interposed between the ruptured end of the ligament and its web page of bony attachment.
Carpometacarpal jointThe bony anatomy of the carpometacarpal (CMC) joint includes the 5 metacarpal bases that articulate with the trapezoid, trapezium, capitate, and hamate (in that order) from the radial side of the hand to its ulnar aspect. The CMC joint is a moderately fixed joint section because of the articular congruity of the joint surfaces, with the metacarpal bases acting like concave receptacles to the distal carpal row, and because of the strong interosseous and extrinsic ligament complicated.
The palmar and dorsal ligaments are dissimilar, with the palmar ligaments being better. The scaphoid acts as a link between the proximal and distal carpal rows. The extensor and flexor tendons move over this articular area but add no strength to the CMC joint because the bases of the metacarpals dislocate dorsally relative to the distal carpal row.
the first CMC joint (also referred to as the first metacarpotrapezoid joint) is a extremely mobile saddle joint, with articular surfaces that are reciprocally concavoconvex. crucial mushy-tissue toughen for this primary CMC joint is the deep ulnar or anterior indirect ligament, which runs from the volar beak of the metacarpal to the tubercle of the trapezium. This ligament may also be ruptured, but it tends to be avulsed with a bit of bone (Bennett fracture-dislocation).
PreviousNextPathophysiologytraumatic pressure applied to the hand can be transmitted to bone, gentle tissue, nerves, and vascular structures. for the reason that structures of the hand are on the subject of the surface and close to each different, damage regularly ends up in a combination of fractures, dislocations, and mushy tissue damage.
The DIP and PIP joints both have lateral ligaments and a fibrous volar plate. widespread dislocations are posterior or lateral. standard forces leading to DIP dislocations include a jamming blow to the tip of the finger. Forces that repeatedly result in PIP joint dislocation embody axial loading or hyperextension. Lateral dislocations may result from radial- or ulnar-directed force on the joint.
Dislocations of finger MCP joints are uncommon and frequently are trapped through the surrounding ligaments, during which case surgical relocation is necessary. MCP or palmar dislocations happen when a hyperextension motion occurs with rotation. The finger is bent again towards the top of the hand and is twisted all over the injury. The finger may have been pushed, or compressed, throughout the injury. MCP dislocations are most often related to fractures.
In thumb MCP joint dislocations, the mechanism encountered most often is hyperextension that results in volar dislocations. a significant lateral force can disrupt the collateral ligaments, leading to instability. Gamekeeper’s (skier’s) thumb often results from a fall onto the hand with the thumb in abduction (as when the hand grips a ski pole).[1]
CMC joint dislocation will not be all the time a excessive-power harm. Identification includes careful prognosis of delicate findings on radiographs and may just require additional radiographic views. overlooked diagnosis of carpometacarpal dislocation may end up in vital morbidity.
PreviousNextEtiologyHand dislocation is caused by the next:
sports injuries (frequently involving contact sports activities or a ball forcefully hanging the tip of the finger)Occupational injuriesFallsTraffic collisionsSport-particular biomechanicsDislocations of the PIP and DIP joints of the hand more than likely occur most frequently in basketball and football. In basketball, the usual mechanisms embrace being struck by means of the ball, catching a finger on the rim, or contact with another participant. In soccer, the finger is also caught on a jersey, slapped against a helmet, or crushed between some aggregate of gamers, gear, and the bottom. Linemen and protective avid gamers are at best chance. In both sports activities, return to play virtually always requires that the harm can also be splinted stably to allow a power grip.
Dislocations of the MCP and basilar CMC joints happen most repeatedly with falls on the outstretched hand (so-referred to as FOOSH harm) or the flexed supinated wrist. With this extension vector, the forces are transmitted up in the course of the carpus.
accidents and dislocations of the thumb, the MCP joint, and the CMC basilar joint repeatedly happen in falls with the thumb in abduction. Examples of this sort of harm embody a fall on the gloved hand in baseball or utility of an abduction drive to a flexed thumb whereas the hand is greedy an object—as in snowboarding injuries, when the pole influences the proximal phalanx tearing the radial collateral ligament. this happens when the wrist is extended at the time of the injury.
PreviousNextEpidemiologyThe annual incidence of all types of dislocations within the hand is roughly 67,000 in the united states. Most hand dislocations are sports activities or occupational injuries, with a lesser number sustained in falls and traffic collisions (every so often associated with airbag deployment).[2, 3, 4, 5, 6]
a lot of these accidents are dislocations on the PIP joint, for the reason that better ROM of this joint makes it extra vulnerable to harm. Of the PIP dislocations, most are dorsal.[7] Volar dislocations of the PIP joint are a lot less in style, more difficult to cut back, and associated with more problems. DIP joint dislocations are also distinct, nearly all the time dorsal, and continuously open.
along with PIP and DIP joint dislocations, MCP and CMC joint dislocations also happen, though less often.[3, 8, 9] The MCP joint of the 4 fingers usually dislocates posteriorly (simple kind) but can, on rare occasions, turn into entrapped between the palmar fascia and the palmar plate and change into irreducibly dislocated.[10] CMC joint dislocation is a disabling injury, which is frequently dorsal and is also related to fractures of the bases of the metacarpals.
Transcarpal fractures in kids are uncommon, but the emergency medical doctor must be cognizant that they do happen.
PreviousNextPrognosisAnatomic restoration of dislocated joints is imperative for achieving just right long-time period outcomes. correct and stable reduction, early fixation, and initiation of ROM exercise are essential. Dislocations can lead to osteoarthritis, compression neuropathies, and carpal tunnel syndrome. extra incapacity from chondrolysis, carpal instability, and annoying arthritis might also occur.
Median or ulnar neuropathy can happen from direct nerve compression or increased power within the median or ulnar nerve canals.[11] analysis of the patient’s nerve standing is mainly necessary in the early analysis of carpal dislocations.[12] Grip energy have to be tested prior to and after discount.
The prognosis is just right for simple PIP dislocations and most DIP dislocations, in addition to for volar dislocations with the significant slip intact (rotatory subluxations). incessantly, some lack of ROM happens, however with sufficient rehabilitation, a useful vary can also be maintained.
The prognosis is honest for volar dislocations with avulsion of the significant slip if the analysis is made on the time of preliminary evaluation and right kind treatment initiated; alternatively, the prognosis is truthful to negative for dorsal fracture-dislocations.
The prognosis is negative for any dislocation that is incompletely reduced for quite a lot of days and may be very poor for a dorsal fracture-dislocation or a volar dislocation with central slip harm if the analysis shouldn't be made and applicable remedy instituted early during the damage.
The prognosis is excellent in most MCP joint and CMC joint dislocations which can be treated early. lengthen in diagnosis and treatment may just progressively irritate the prognosis. lengthy-term sequelae of hand dislocations with damage to the joint surface embrace instability, ankylosis, and arthrosis.
PreviousNextPatient trainingAll athletes in excessive-possibility sports should be aware of to have vital finger accidents evaluated and handled with the aid of the staff health practitioner or coach at the time they happen. This helps to steer clear of one of the morbidity from fracture-dislocations, boutonniere accidents, and incompletely diminished dislocations. in addition, all athletes who sustain these injuries must be made aware of the significance of timely follow-up, of the expected length of immobilization, and of the rehabilitation plan, targets, and timetable.
For patient schooling instruments, see broken Hand, broken Finger, and Hand accidents.
PreviousProceed to clinical Presentation , Hand Dislocation





0 comments:
Post a Comment
Note: Only a member of this blog may post a comment.